
Hims vs Tempus AI
Value Chain Analysis

This is an update of my original Hims deep dive and Tempus AI deep dive.
Hims and Tempus are building the same machine from opposite ends of medicine: one from your phone, one from the hospital. The only thing keeping them apart is incentives.
Strip away the surface and Hims and Tempus are doing the same thing: building an Ontology of human biology. Not a drug, not a test, not a subscription, but a continuously improving model of the world they operate in, assembled from proprietary data no one else holds.
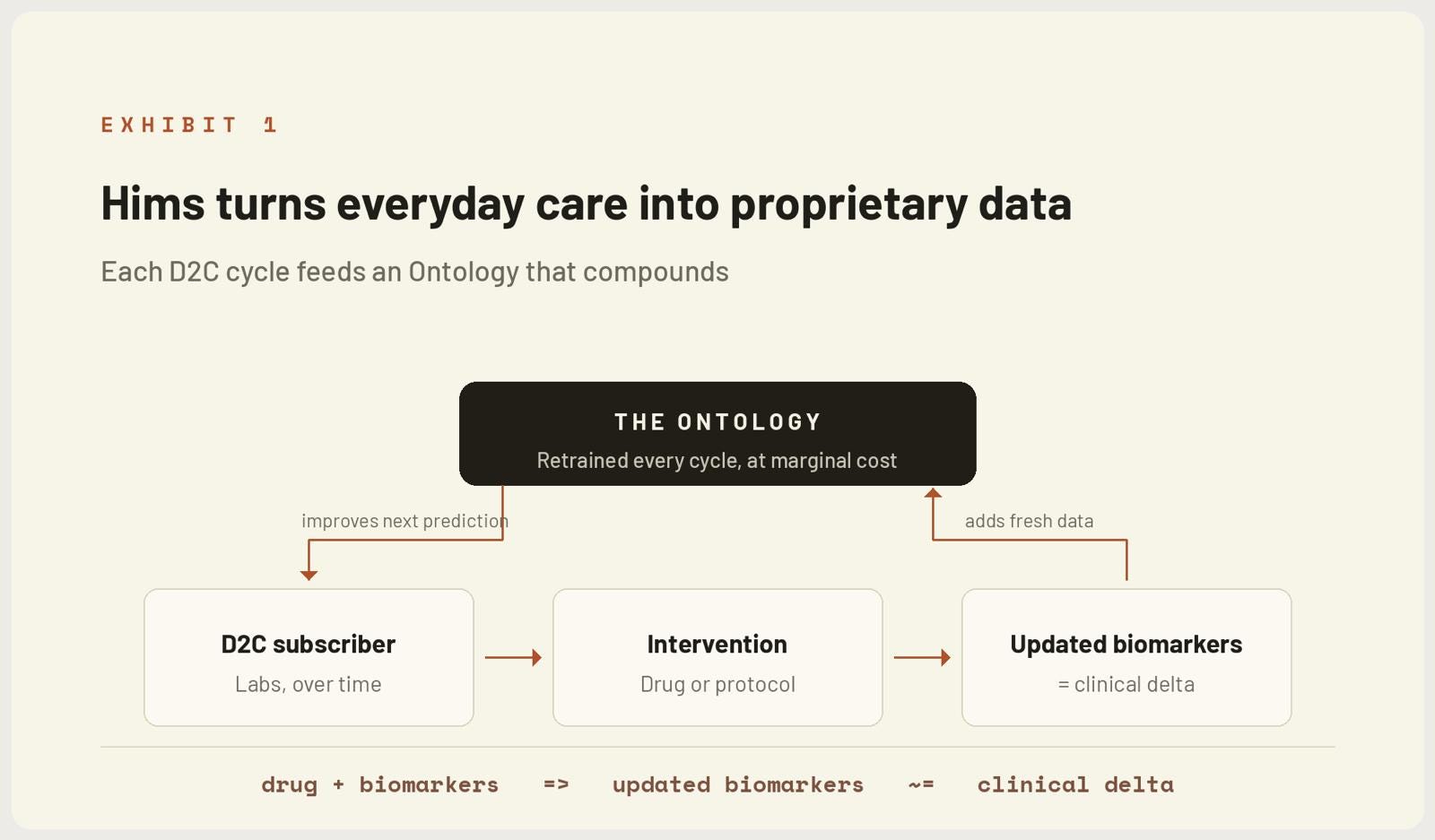
Hims sources its Ontology from the D2C channel. Every subscriber is a node, and as Hims expands Labs, it harvests more biomarkers about each one over time. The longer you stay, the denser your longitudinal record becomes. That density is the raw material.
What the network is actually learning is a function. It observes what input, a drug, a peptide, a protocol, modifies which biomarkers, in which direction, and how that change maps to a clinical outcome. On a first principles basis, the entire thesis compresses into one line:
drug + biomarkers ⟹ updated biomarkers ≈ clinical delta
Run that loop across millions of subscribers and you no longer have a pharmacy. You have a model that knows, before you act, what a given intervention will do to a body like yours.
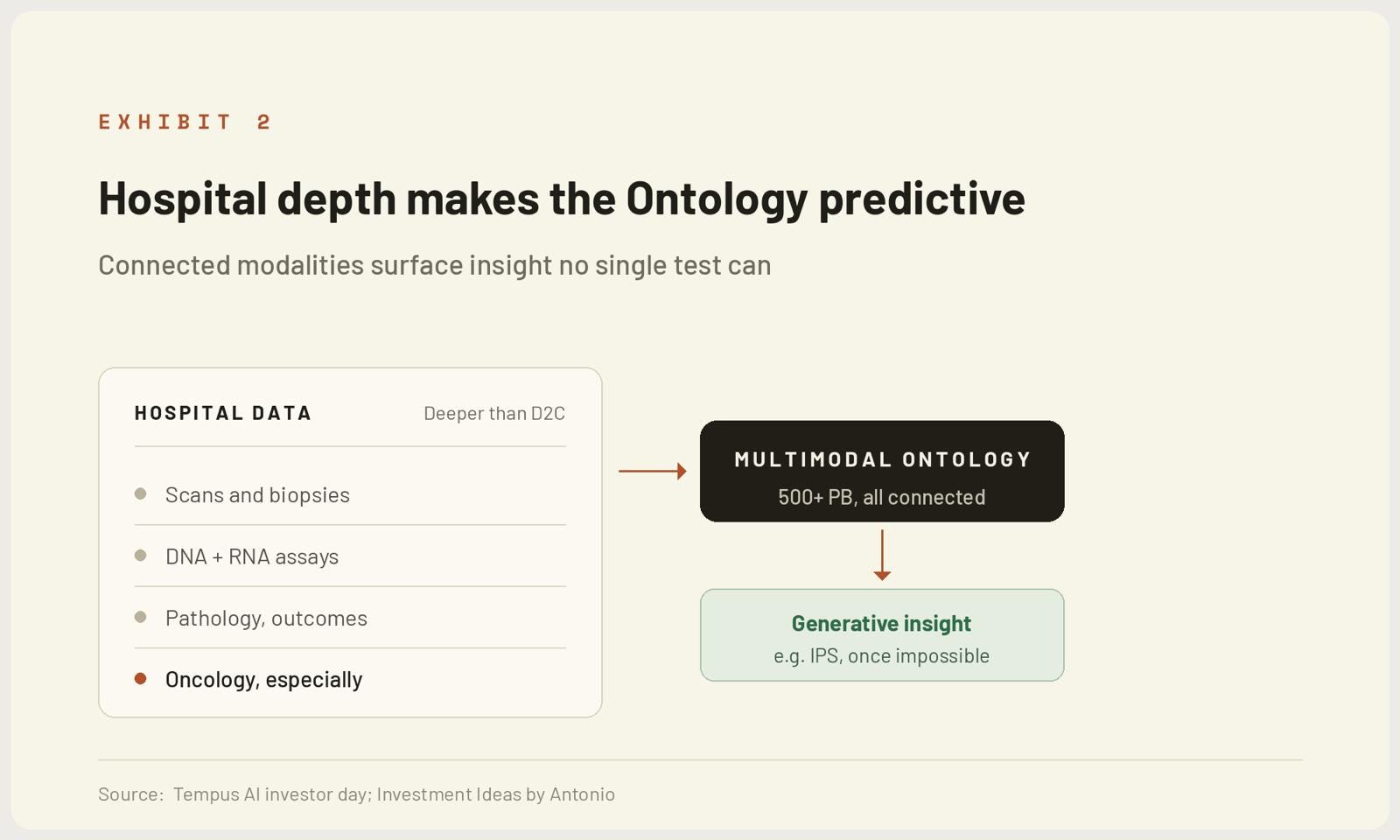
Tempus is building the identical Ontology from the opposite end of the system. Its data does not come from a subscriber typing into an app. It comes from the clinical core: scans, biopsies, genomic assays across DNA and RNA, pathology, treatment records, response and adverse event data, all connected.
The consequence is depth. Hospitals currently go deeper than any D2C channel can, so Tempus inherits that depth by default. Its richest seam is oncology, over 4.5 million sequenced samples and 400,000 plus deeply multimodal records, where every layer of a real patient's cancer trajectory is wired to every other.
And depth is what lets the model generalise. As I covered in the deep dive, once the Ontology is dense enough, AI begins predicting things that were previously impossible to compute. The immune profiling score (IPS) is the proof of concept. It took a team of computational scientists years to build, it goes underneath the standard biomarkers, and it predicts who actually benefits from immunotherapy. IPS is not the achievement. It is the first output of a machine that will print the next thousand insights like it.
Here is where the framework I have been building for years applies directly. Both companies run the same loop,
drug + biomarkers ⟹ updated biomarkers ≈ clinical delta
and both feed every result back as proprietary data that sharpens the next prediction. As the Ontology approaches exhaustiveness and AI scaling laws keep doubling the model beneath it, the system crosses a threshold. It stops describing what happened and starts being biologically predictive.
It becomes a machine that prints insight at the marginal cost of inference, a Singularity Scaler, where the thing produced decouples from the thing spent and the gap widens as compute scales.
The endpoint is identical for both: an Ontology that tells you what to do before you get sick. Prevention computed in advance, rather than disease treated in arrears.
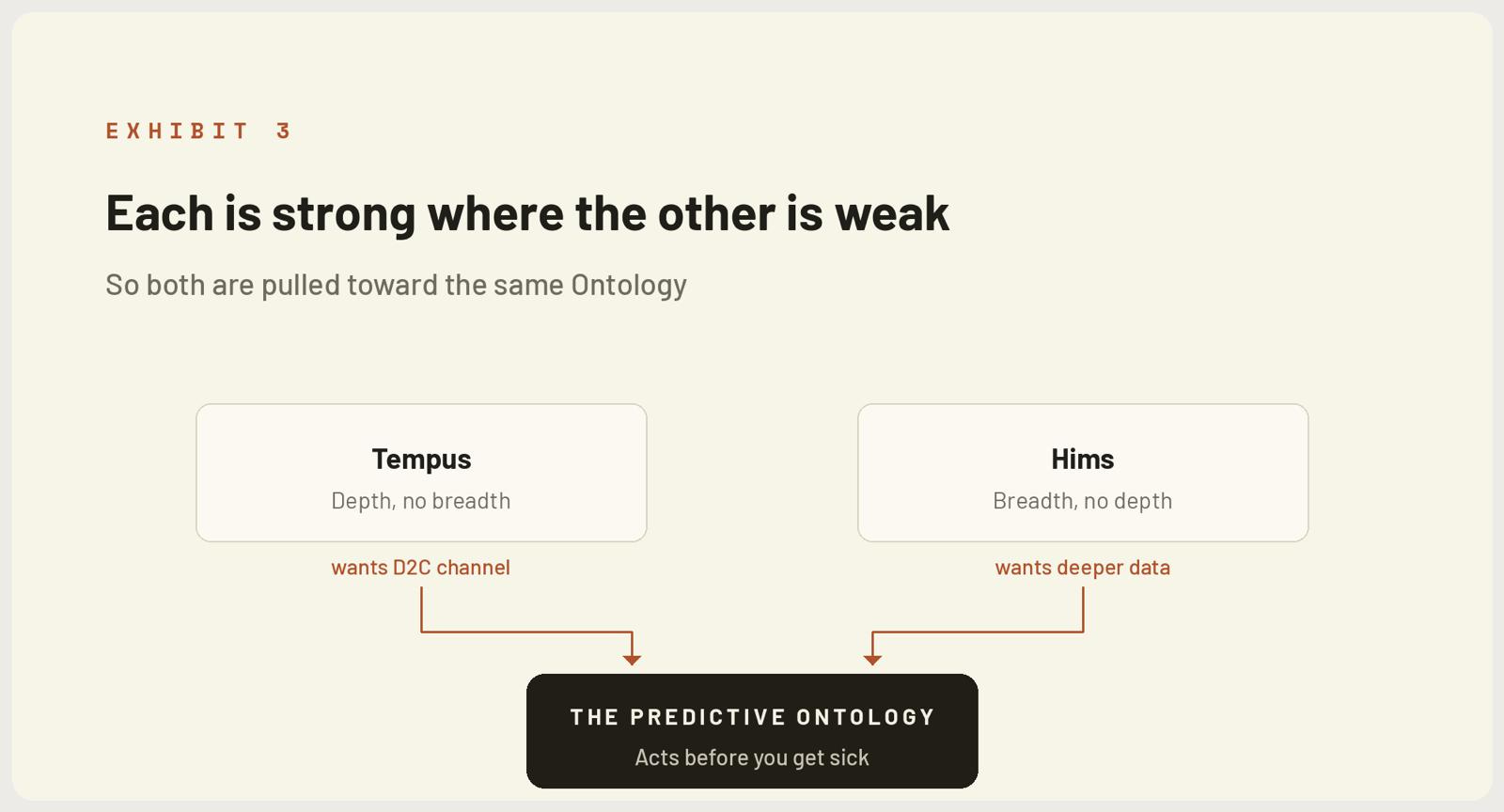
But they arrive carrying opposite shapes. Tempus has depth, Hims has breadth. Tempus knows end customers the atomic level through the hospital. Hims knows a its end customers continuously through the phone. And because each is strong exactly where the other is weak, both have a mechanical incentive to move toward the other:
Tempus wants the D2C channel, wearables, direct to patient pipes. Not just more data, but a delivery path that bypasses its dependency on the hospital to action anything.
Hims wants deeper data, hospital grade depth it can pour through the D2C infrastructure it already owns, to deliver sharper insights to the subscriber it already has.
This is Ontology Velocity pulling two companies toward the same point from opposite directions.
If you accept that both are building predictive Ontologies of human biology, then at the level that matters they are the same company. What separates them today is not technology, nor even the data type. It is incentives, and incentives are inherited from the rails each one runs on.
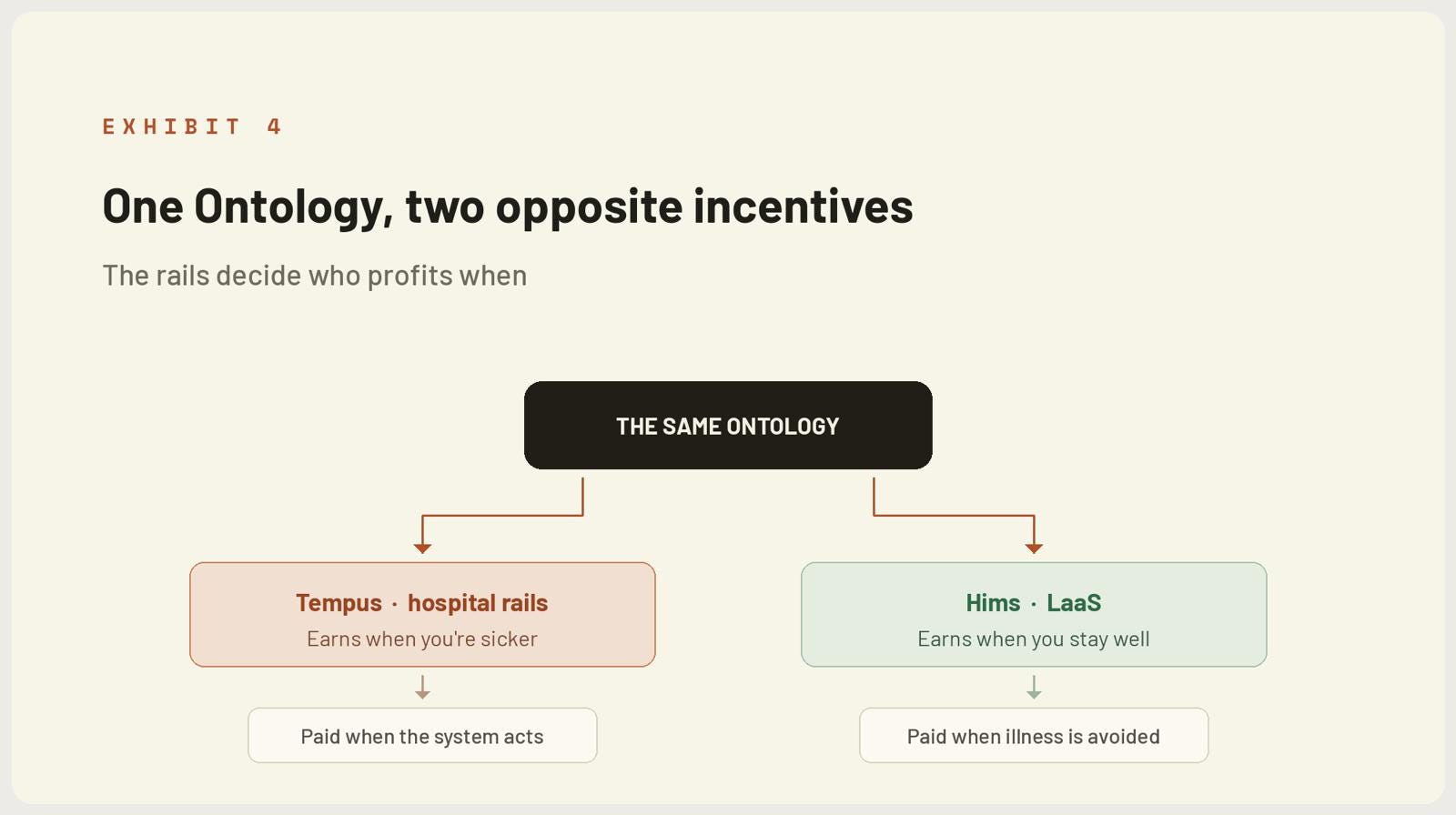
Tempus draws its data through the hospital, and the hospital does not make money if you don't show up. So even though Tempus itself profits by delivering more and better insight at a lower cost, those insights get actioned through an infrastructure whose economics improve the sicker you are. The Ontology points toward prevention. The system it plugs into is paid for disease.
Hims runs on the opposite incentive. Its model is longevity as a service, LaaS, and under LaaS the company makes more money the longer you stay well. The subscription is the alignment. Keep the customer healthy and optimising, and lifetime value compounds.
Same Ontology, opposite reflexes. One is paid when the system acts on illness. The other is paid when the customer avoids it.
Whatever happens next, the base case holds: Tempus is converting the hospital into a set of generative AI algorithms. The ECG read, the pathology call, the immunotherapy match all become model outputs rather than human ones. And that conversion is precisely the thing that can, over time, change the incentives above. Once the model can tell you years in advance who has the heart attack, prevention becomes the cheaper path, and systems eventually follow the cheaper path, though the reimbursement machinery that resists it bends slowly, so this is a destination, not the present.
From there the tree splits.
In the first branch, Tempus builds its own D2C infrastructure, wearables, direct to patient delivery, and pivots toward LaaS itself. In that world it stops being adjacent to Hims and becomes a competing Ontology: same shape, same incentive, fighting for the same patient.
In the second, Tempus does not build D2C. Then it becomes the engine distributed through D2C channels like Hims, the depth layer that companies with breadth license and pour through their own pipes. Lefkofsky has already told us which way the wind blows: customers increasingly don’t just want the data, they want to build their models on the platform.

Either branch resolves the same way at the consumer level, and this is what anchors the whole thesis: customers do not want to go to hospitals. D2C channels will keep climbing the acuity ladder, from primary care toward urgent care, and the onset of robotic surgeons collapses much of what currently forces a hospital visit at all. The depth that only the hospital can capture today migrates, over time, to the channel the patient actually prefers.
⚡ If you enjoyed the post, please feel free to share with friends, drop a like and leave me a comment.
You can also reach me at:
Twitter: @alc2022
LinkedIn: antoniolinaresc
Great reading Antonio, always exceptional education , much appreciated for your works always
Gracias por el trabajo.
Tres tonterías que me rondan la cabeza:
1.- Coincido en la convergencia hacia DTC. Eso lo veo claro; TEM se está ahogando en la oncología.
2.- Considero más fácil que HIMS vaya adquiriendo e integrando de manera natural nuevas verticales a que TEM salga abruptamente del sistema sanitario "duro" en el que está fuertemente integrado y comience de cero una DTC.
3.- Como consumidor/paciente pienso que lo ideal sería que una DTC con buena distribución tuviera la calidad de los datos de TEM y, a veces, los movimientos que se producen son los que van dirigidos al beneficio del cliente final